Article Text

Statistics from Altmetric.com
New government legislation is necessary to ensure full transparency of industry payments in the UK’s healthcare. A first step should involve challenging the industry-driven discourse that allows company payment disclosures to be inconsequential for managing conflicts of interest.
The ‘Independent Medicines and Medical Devices Safety Review’, led by Baroness Julia Cumberlege and published in 2020, expressed concerns about the impact of financial conflicts of interest (COIs).1 Using high-profile cases of avoidable harms, it highlighted that payments that clinicians receive from drug or medical device manufacturers often lack transparency and ‘may influence their practice, and the course of action they recommend to patients, such as preferentially using particular procedures or drugs’.1
The policy impetus generated by the Cumberledge review resulted in a government consultation, held in 2023, on a legislative framework to make industry payments to healthcare professionals and organisations more transparent.2 One key proposal was the ‘expansion’ of Disclosure UK (box 1), the payment database managed by the Association of the British Pharmaceutical Industry (ABPI), and the central pillar of the UK’s disclosure system for drug companies.2
Industry self-regulation and Disclosure UK
Companies subscribing to the Association of the British Pharmaceutical Industry (ABPI) Code report research and non-research payments on the online platform called Disclosure UK.
Companies define research payments as relating to their non-clinical studies, clinical trials and non-interventional prospective studies. They are aggregated per company, with no recipients named.
Non-research payments cover collaborative working, donations and grants, consultancies, and event sponsorships. Since 2019 all healthcare organisations receiving payments must be named. Since 2020 the ABPI has recommended naming healthcare professionals, but some payments are still disclosed without names.
Only collaborative working has information about intended payment goals but without the requirement to disclose associated products.
However, the limitations of the current system mean that expanding it will not ensure transparency. Although Disclosure UK is ranked among the top industry-run disclosure systems internationally,3–5 it captures adequately only some payments, leaving others overlooked or hidden. The uncertainty regarding whether payments were made and to whom undermines the ability of policymakers, regulators and healthcare providers to detect COIs, posing unmitigated risks to patient care.
To meet a core recommendation of the Cumberlege review1—to improve the transparency of financial interactions with industry—the government should develop new legislation, drawing on the experience of other developed countries that have either created bespoke Sunshine Acts or introduced payment disclosure requirements to their existing healthcare legislation (box 2).3–6 Contrastingly, reforming self-regulation or creating a ‘mixed’ legislative/self-regulatory system is unlikely to bring significant improvement.
Industry self-regulation versus payment transparency legislation: an international context
Self-regulation is the dominant approach to disclosure in developed countries: most of Europe, Australia, Canada, Japan, New Zealand.
Countries with comprehensive Sunshine legislation: Italy (passed in 2022 but not yet enforced), France, the USA.
Countries with varying levels of payment disclosure provisions added to existing healthcare legislation: Denmark, Estonia, Greece, Hungary, Latvia, Lithuania, Portugal, Slovakia, Romania, Turkey.
Countries with ‘mixed systems’ where legislation allows, like under self-regulation, the industry to decide and implement disclosure rules: Belgium, Finland.
Divergent interests and transparency paradox
The UK government declares that it seeks to protect the public interest, including patient health, by ‘encouraging industry-led initiatives that meet the minimum statutory requirements’.2 However, this approach overlooks the fundamental divergence of interests between the public and industry regarding transparency.
Trade bodies governing self-regulation, such as the ABPI or its ‘parent’ organisation, the European Federation of Pharmaceutical Industries and Associations (EFPIA), use transparency primarily to protect the industry’s reputation (box 3). For them, making payments publicly available—but not necessarily accessible, analysable or meaningful—is sufficient to meet the reputational goals.
Industry payment disclosure and reputation management
The Association of the British Pharmaceutical Industry (ABPI) and European Federation of Pharmaceutical Industries and Associations (EFPIA) emphasise enhancing the industry’s reputation as a key disclosure goal.
‘The industry recognises that transparency is an important means of building and maintaining confidence’ (ABPI Code, p.7).
‘Self-regulation includes the concept of a continuous challenge for us to exceed society’s expectations and openness regarding suggestions from others on how we might further strengthen confidence in our industry and our behaviour’ (EFPIA Code, p.9).
While EFPIA acknowledges conflicts of interest, payment disclosure does not focus on managing them but, instead, emphasises boosting confidence in industry collaborations.
‘[I]nteractions between the industry and [healthcare professionals and organisations] can create the potential for conflicts of interest’ (EFPIA Code, p.12).
‘[D]isclosure contributes to the confidence of stakeholders in the pharmaceutical industry’ (EFPIA Code, p.12).
Conversely, the National Health Service (NHS),7 and the National Institute for Health and Care Excellence (NICE)8 recognise Disclosure UK’s potential role in detecting COIs—a crucial first step in preventing their associated harms.6 9 For example, NICE expects that an application to sit in an advisory committee will be followed by a review of Disclosure UK ‘to identify if any other interests need to be declared [beyond those declared by the applicant]’.8
Uncertainty in payment disclosure
To become a genuine tool in managing COIs, disclosure reporting must follow certain minimum quality standards that ensure reliable tracing of all payments from all companies. One of the most influential formulations of such standards includes the criteria of disclosure accuracy, consistency, completeness and searchability specified by Lo and Field.9
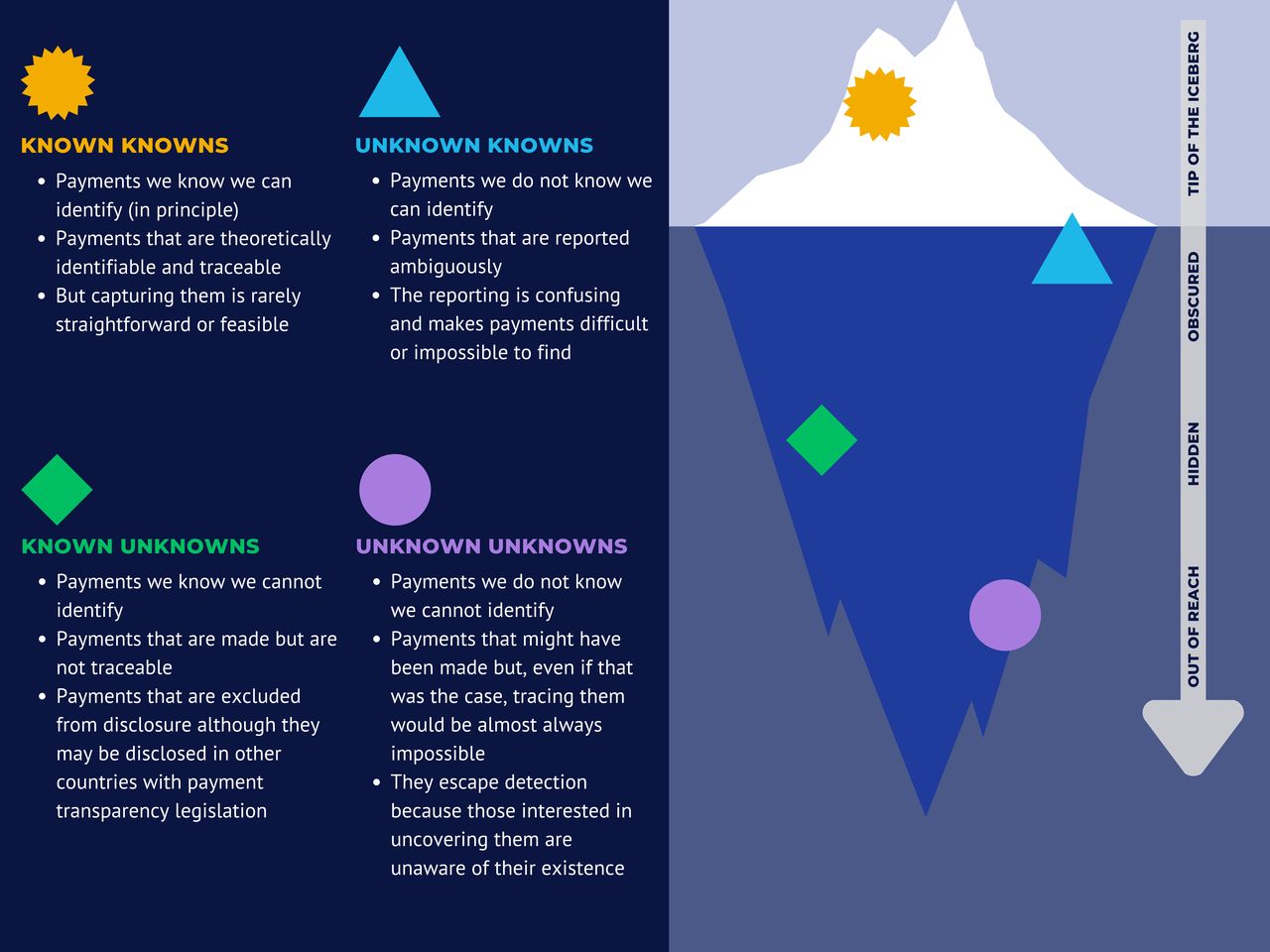
Nevertheless, Disclosure UK fails to meet these criteria, which we demonstrate by assigning industry payments to the four categories from the Rumsfeld Matrix, inspired by remarks made by the US Defence Secretary Donald Rumsfeld on the gaps in intelligence about alleged weapons of mass destruction in Iraq.10
‘Known knowns’—payments identifiable, at least theoretically, through Disclosure UK.
‘Unknown knowns’—payments whose existence is uncertain given the confusion in companies’ disclosure records.
‘Known unknowns’—payments made but not traceable in Disclosure UK.
‘Unknown unknowns’—payments that remain undetected because their existence is not deducible from companies’ records.
Cumulatively, these layers of uncertainty mean that the public only sees the ‘tip of the iceberg’ of payments, with an unknown share being obscured, hidden or completely untraceable (figure 1). The lack of full and reliable information about industry financial ties undermines—if not eliminates—possibilities for establishing the existence, extent and effects of any associated COIs.

The iceberg of uncertainty in payment reporting in Disclosure UK. Source: own research. Figure created using Canva.
The uncertainty arises from an interplay between the imprecise disclosure rules from the ABPI Code, their inconsistent implementation by companies, and the poor quality of the Disclosure UK data.5 11 But the uncertainty is not unavoidable—it can be prevented using provisions from payment transparency legislation developed elsewhere (table 1).3 4
The mechanisms of uncertainty in Disclosure UK and solutions from payment transparency legislation
Denmark—Health Act of 2014 and Executive Order No. 1153
Estonia—Medicinal Products Act of 2005 (provisions from 2013)
France—Law Number 2011–2012 (Loi Bertrand)
Hungary—Act XCVIII of 2006 on the General Provisions Relating to the Reliable and Economically Feasible Supply of Medicinal Products and Medical Aids and on the Distribution of Medicinal Products (provisions from 2011)
Latvia—Regulation no 378 on Advertising Medicinal Products Procedures for Advertising Medicinal Products and Procedures by Which a Medicinal Product Manufacturer is Entitled to Give Free Samples of Medicinal Products to Physicians
Lithuania—Law on Pharmacy and Ministerial Order no V-1537/2000
Portugal—Decree Law 20/2013 and 128/2013
Romania—Ministerial Orders 194/2015 and 874/2015
Slovakia—Act No. 362/2011 on Medicines and Medical Devices
USA—Physician Payments Sunshine Act (Sunshine Act)
Known knowns
The ‘known knowns’ of payment disclosure encompass payments identifiable, at least theoretically, through Disclosure UK. They have been scrutinised across healthcare professionals,12 general practices,13 NHS Trusts14 and professional organisations,15 highlighting potential conflicts between industry funding and the imperative of high-quality patient care.
However, these disclosures are ‘known knowns’ only to those well-versed in the intricacies of Disclosure UK and capable of undertaking forensic research.
Consider NHS Trust A contributing to an NICE technology appraisal.14 One might expect that searching in Disclosure UK would reveal a complete picture of the trust’s drug company funding. Yet, without clear naming rules and unique recipient identifiers, such as those mandated by the US Sunshine Act (table 1), companies can use multiple names and abbreviations. Some can also identify the trust indirectly through its constituent hospitals, departments or clinics. Conversely, some payments may be misattributed, which becomes evident through cross-referencing Disclosure UK entries with the trust’s official address information.
These challenges in accurately identifying payment recipients pervade the entire database.5 13 16
Unknown knowns
The ‘unknown knowns’ involve payments whose existence is uncertain due to reporting inconsistent with the disclosure rules.
Take, again, NHS Trust A—to check its ties comprehensively, NICE must account for potentially misreported payments, both within and outside of Disclosure UK.
One issue, also enabled by the lack of unique recipient identifiers, is payments misattributed to the wrong organisations or persons sharing the same name.5 14 16 Moreover, unlike in, for instance, France’s Loi Bertrand (table 1), recipients subject to reporting are not categorised. Consequently, payments to individuals are sometimes mistakenly reported in the database section covering organisations.16 Similarly, some payments to patient organisations are reported in Disclosure UK, although they belong in a separate system.16 Conversely, from 2015 to 2018, over 10% of payments listed under patient organisations should have been reported in Disclosure UK.17 Confusingly, some payments to the same organisation may be reported in both systems concurrently, creating uncertainty around potential duplication and totals received.
Known unknowns
The ‘known unknowns’ include ties whose existence is acknowledged in Disclosure UK, but where disclosure rules permit concealment, exacerbated by inconsistent company practices.
For instance, Consultant B, invited to an NICE appraisal, cannot have their COI declaration verified fully through Disclosure UK, as the database ‘discloses’ most payments ‘in aggregate’—without naming recipients (box 1).
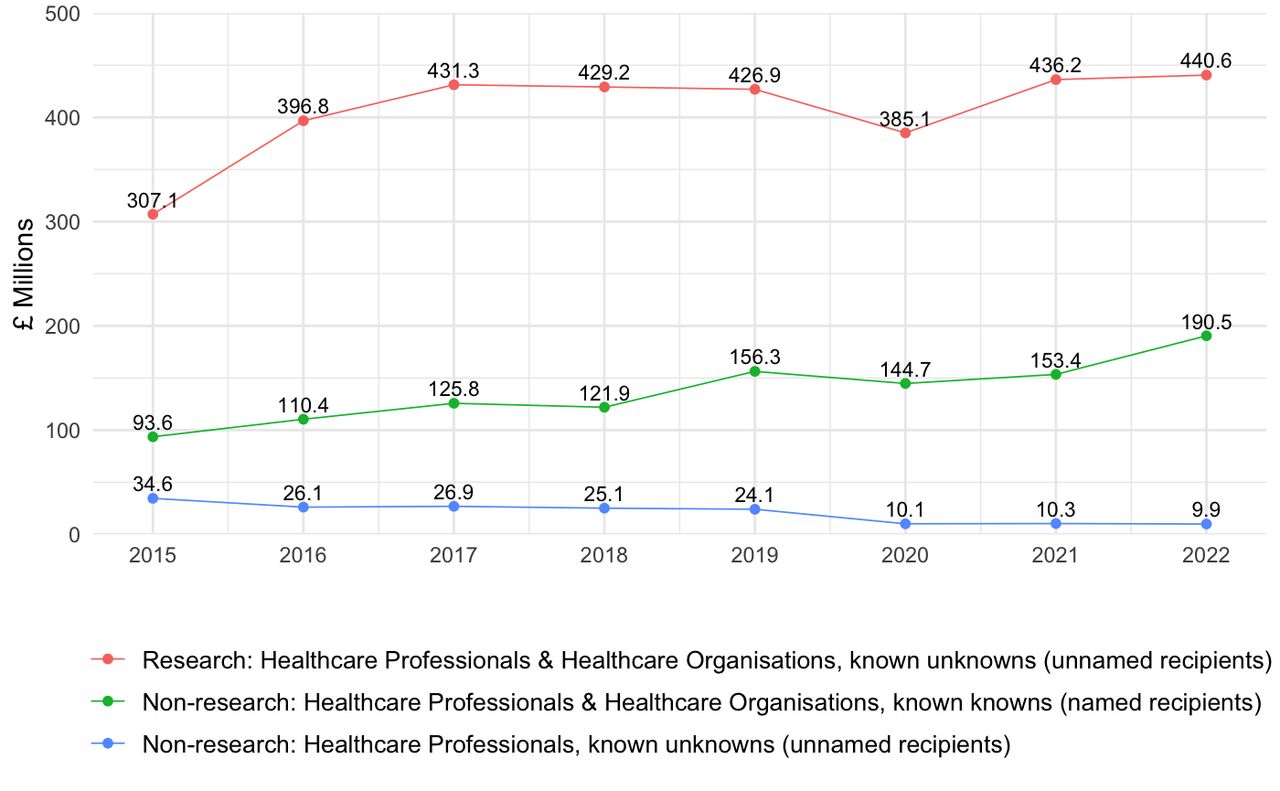
Payments to healthcare professionals and organisations for participation in companies’ research, including clinical trials, are reported as annual lump sums without detailing recipients or activities (box 1).4 From 2015 to 2022, research payments exceeded non-research payments to named recipients threefold (£3.3 billion vs £1.1 billion), constituting 72% of all payments (figure 2). High shares of research payments, including those by Allergan, Bristol Myers Squibb, and AstraZeneca (at least 90% for the entire period), are claimed as genuine research investment, but may reflect a flexible interpretation of what qualifies as research and research-related payments, a practice permitted by the ABPI Code.4

{kind=link}
{kind=link}
Trends in the value of ‘known knowns’ and ‘known unknowns’ in Disclosure UK. Aggregate – payments reported without named recipients. Payment values are adjusted for inflation using the CPI index obtained from the Office of National Statistics.The figure excludes payments worth £5.2m which some companies made to healthcare organisations without identifying them, a known unknown. The possibility of aggregate reporting of payments to healthcare organisations was removed by the ABPI in 2019. Source: Disclosure UK databases obtained from the Association of the British Pharmaceutical Industry website https://search.disclosureuk.org.uk/Public/DownloadFullDataSet. The data was analysed in Microsoft Excel and visualised in RStudio (version 2024.04.2).
Payment transparency legislation mandates the disclosure of research payments in several countries (table 1).4 However, the UK government endorses the industry’s stance that secrecy is vital for investment, proposing to exempt ‘commercially sensitive information’ from disclosure.2
Despite the size of unknowns generated by research payments, the ABPI highlights a different issue caused by healthcare professionals refusing consent for companies to disclose their non-research consultancies and event sponsorships. Yet, this form of aggregate reporting represented merely 4% of the total (£0.2 billion vs £4.5 billion) between 2015 and 2022 (figure 2). The ABPI’s explanation emphasises insufficient commitment to transparency from individual recipients,18 while downplaying the impact of varying company practices, as suggested by disclosure rates ranging from nearly 100% to 15% among major UK companies.12
Since 2020 the ABPI has recommended that companies do not actively seek consent from healthcare professionals, although they can still ‘raise objections’ to the disclosure of their non-research payments.19 20 By 2022, these aggregated payments had fallen to nearly £9 million, a considerable drop compared with 2019. While celebrated as a success by the ABPI,19 the new recommendation underscores two critical flaws in self-regulation—difficulty in enforcing non-mandatory guidance across companies and the fact that, in the European legal environment, individual non-disclosure can ultimately be eliminated through legislation or other government mandate over-riding data privacy rights.3
Additionally, Disclosure UK does not mention—and therefore implicitly excludes—non-research payments and other interests covered in some countries with payment transparency legislation (table 1). For example, the US Sunshine Act covers ownership and investments and small hospitality payments known to be widespread and influence prescribing.21
Further, while Disclosure UK includes recipients involved in prescribing or managing prescription medicines, France’s Loi Bertrand covers a broad set of ‘players in the health field’, including media organisations and media and social ‘influencers’. Combined with the user interface from the independent eurosfordocs.fr platform, this wide-ranging data has enabled tracing COIs which can interfere with both healthcare standard setting and delivery.3 4
Yet another known unknown is the lack of information on how the money is spent by recipients. Contrastingly, transparency legislation mandates brief payment descriptions in several European countries, including the names and/or dates of industry-sponsored meetings.
Finally, Disclosure UK does not cover medical device companies, which use a separate self-regulatory system.22 However, they are often covered by transparency legislation, including Loi Bertrand, which also extends to manufacturers of veterinary products and cosmetics.
Unknown unknowns
The ‘unknown unknowns’ represent financial connections that may exist but remain unreported because the companies involved either do not subscribe to or breach the ABPI’s disclosure rules.
For example, when using Disclosure UK to assess the COIs of NHS Trust A or Consultant B, NICE must consider potential undisclosed ties, which are nearly impossible to trace even when triangulating with institutional disclosures.
One concern is payments potentially made by companies not signing up to the ABPI Code and therefore not obligated to disclose their payments.5 Despite the ABPI’s claims of few such companies, notable exceptions, like Vertex, exist.5
Further, the Prescription Medicines Code of Practice Authority (PMCPA), the ABPI’s self-regulatory body, ruled that since 2016 seven companies breached the ABPI Code by failing to report some of their payments in Disclosure UK. The most egregious was Novo Nordisk’s failure to report around 500 payments worth £7.8 million to over 150 UK healthcare professionals and organisations.23 Companies typically highlight that unreported payments arise from human error, internal process failures or misunderstanding of the disclosure rules.
As companies often struggle to trace all missing payments, the PMCPA rulings reveal only a minimum extent of unreporting.5 23 The possibilities for discovering unreporting are constrained by the PMCPA lacking independent investigative powers,23 relying instead on voluntary admissions by companies or evidence presented by complainants, typically healthcare professionals and industry whistleblowers.24
Redefining disclosure and addressing uncertainty
The fact that the government is considering expanding Disclosure UK reflects its acceptance of an industry-driven discourse that conceals the divergence of interests between the industry and the public regarding transparency. This discourse does not prioritise exposing COIs but protecting the industry’s reputation through the paradoxical concept of ‘aggregate disclosure’3 4 and the silence around donors, payments, and recipients disclosed elsewhere.
Once this discourse is recognised, it becomes clear that the uncertainty can only be addressed with transparency legislation using the international experience (table 1). Responding to the ‘known unknowns’ of Disclosure UK requires expanding disclosure rules to new payments, recipients, and industries. New rules regarding recipient identifiers, categories and payment descriptions are necessary to eliminate the ambiguities generating the ‘known knowns’ and ‘unknown knowns’.
A bespoke Sunshine Act would likely eliminate the uncertainty most comprehensively (table 1), while offering awareness-raising and educational opportunities across stakeholders involved in industry collaborations. However, the alternative route of extending the existing healthcare legislation might be more pragmatic politically. Notably, the transparency provisions included in the Health and Care Act 2022 following the Cumberlege Review could inform policy solutions more quickly and without triggering industry opposition that would likely surround a Sunshine Act proposal.
Irrespective of the chosen approach, it should be combined with standardising company disclosure practices through precise and regularly updated implementation guidelines. This needs to be reinforced through continual and transparent monitoring, supported by companies funding independent disclosure research, similar to the Truth Tobacco Industry Documents database.25 Heavy fines are also needed to deter substandard reporting, with any collected fines supporting compliance efforts.
These transparency gains cannot be achieved under ‘mixed’ legislative/self-regulatory systems (box 2). Most notably, they lack mandated disclosure of research payments and, like in self-regulation, leave the implementation and oversight in the industry’s hands, potentially leading to levels of uncertainty similar or even exceeding those characterising Disclosure UK.3 4
Nevertheless, even enhanced transparency cannot itself address COIs26 and may generate unintended consequences—‘moral licensing’,27 unjustified decrease in trust in physicians,28 or industry surveillance of prescribers.29 Therefore, it should be combined with reducing—or eliminating—industry interactions in professional training, continuing medical education, guideline and policy development.26
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
X @emilyjrickard22
Contributors PO, ER and SM have researched pharmaceutical industry transparency, payment disclosure and self-regulation in the UK and internationally for many years. We have published widely on these issues, including in The BMJ, BMJ Open, Big Data and Society, Sociology of Health and Illness, Health Policy and JAMA Network Open. We have also collaborated with The BMJ several times, including on investigations into drug company payments to NHS trusts and clinical commissioning groups in England. Our work has been impactful, receiving extensive international media coverage and stimulating engagement from the medical profession, regulators, and patient charities. PO is the guarantor of the article.
Competing interests We have read and understood BMJ policy on declaration of interests and have the following interests to declare: PO’s former PhD student was supported by a grant from Sigma Pharmaceuticals, a UK pharmacy wholesaler and distributor (not a pharmaceutical company). The PhD work funded by Sigma Pharmaceuticals is unrelated to the subject of this paper. SM’s partner is employed by ICON, a global Contract Research Organization whose customers include many pharmaceutical companies. ER has nothing to declare.
Provenance and peer review Not commissioned; externally peer reviewed.