Article Text

Abstract
Objectives To develop a core outcome set (COS) for oropharyngeal dysphagia (swallowing disorder) interventions in Parkinson’s disease by agreeing core outcomes and definitions, outcome measurement instruments (OMIs) and time points of measurement for these core outcomes.
Design International online Delphi survey and consensus meetings.
Participants Individuals living with oropharyngeal dysphagia and Parkinson’s disease, family members and caregivers, healthcare professionals and researchers in the field of oropharyngeal dysphagia and Parkinson’s disease.
Methods A long list of outcomes was generated previously through scoping reviews, online surveys and focus groups with key stakeholders. Building on this, an international three-round online Delphi survey was conducted where participants rated the importance of outcomes. In subsequent online consensus meetings, core outcomes, their definitions, OMIs and time points of measurement were agreed on.
Results 90 participants from 21 countries completed all three rounds of the Delphi survey. Of these, 35 participated in a consensus meeting. Six outcomes were agreed as the core outcomes: ‘penetration/aspiration’, ‘aspiration pneumonia’, ‘choking’, ‘oropharyngeal dysphagia severity’, ‘swallowing related quality of life’ and ‘post swallow pharyngeal residue’.
Conclusions The use of a COS in future oropharyngeal dysphagia intervention studies in Parkinson’s disease will facilitate comparative effectiveness research and ensure that outcomes are relevant to all key stakeholders. This should help improve the evidence base for oropharyngeal dysphagia interventions in Parkinson’s disease.
Registration The study was registered prospectively with the Core Outcome Measures in Effectiveness Trials Database on 24 September 2021 (www.comet-initiative.org, registration number: 1942).
- Movement Disorders
- Rehabillitation
- Methods
- NEUROLOGY
- Evidence-Based Practice
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this published article and its supplementary material.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Oropharyngeal dysphagia (swallowing disorder) affects up to 80% of individuals with Parkinson’s disease, yet evidence for effective interventions is limited. A key barrier is difficulty in comparing results of oropharyngeal dysphagia intervention studies due to the use of a diverse range of outcomes, outcome measurement instruments (OMIs) and time points of measurement. One proven solution to this challenge is the development and use of core outcome sets (COS).
WHAT THIS STUDY ADDS
This COS provides a minimum of clearly defined outcomes with recommendations for OMIs and time points of measurement for all clinical trials on oropharyngeal dysphagia interventions in Parkinson’s disease. It also considers some of the challenges associated with COS research.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Measuring and reporting the core outcomes systematically in all future clinical trials on oropharyngeal dysphagia interventions in Parkinson’s disease will improve evidence-based medicine and reduce research waste.
Introduction
Background
Oropharyngeal dysphagia (OD), that is, difficulty in swallowing, represents a clinically and psychosocially relevant symptom among individuals with Parkinson’s disease (PD)1 with a prevalence of up to 80% in this population.2 3 OD can negatively affect the quality of life and nutrition and hydration status. OD can also increase the risk of aspiration and pneumonia, which is considered a leading cause of death in this patient cohort.4–6
Since 2020, eight systematic reviews and one meta-analysis assessing the effects of OD interventions in PD were published.7–14 Despite these efforts to identify the most effective interventions for OD in PD, evidence remains limited. One contributing factor to the weakness of the evidence base is the heterogeneity of applied outcomes and outcome measurement instruments (OMIs) as this makes pooling of results and comparison of treatment effects challenging.7 8 11 12 14 Another point of criticism is that most studies only assess short-term effects of the intervention and that time points of assessments differ widely across studies. Of the nine studies included in the systematic review by Cheng et al,7 all but one assessed the immediate effects of the intervention without conducting a longer-term follow-up assessment. Other reviews report follow-up assessments for some of the included studies at one to a maximum of 6 months.9–11 13 14 This limits the possibility of assessing maintenance effects of interventions, which is particularly important in a neurodegenerative disease like PD.
Another relevant challenge in the evidence base for this area is that outcome selection in clinical trials typically rests with researchers, often without input from other stakeholders.15 This is a common issue.15 16 Treweek and colleagues, for example, found that the outcomes prioritised by people with the health condition and healthcare professionals differ from those chosen by researchers.17 Consequently, the applied outcomes might be less relevant to key stakeholders, such as people with the health condition, who ultimately should benefit from the research results.18 One solution to harmonise outcomes and OMIs, facilitate comparative effectiveness research and increase the relevance of outcomes to key stakeholders is the development and use of an agreed, standardised core outcome set (COS). A COS is a minimum set of outcomes agreed upon by relevant stakeholders. It is recommended that the COS be measured and reported in all clinical trials of a specific health condition. However, it does not restrict or prevent researchers from measuring other outcomes that might be relevant to their research questions.19 20
A search of the Core Outcome Measures in Effectiveness Trials (COMET) initiative database (www.comet-initiative.org) was conducted, and two published COS studies on PD in general, but not on OD specifically, were identified.21 22 Both studies comprise outcomes related to OD but are not specific to OD, and both lack the involvement of experts in OD, such as speech and language therapists (SLTs). However, both studies provide preliminary evidence that OD in PD is relevant, but a specific COS for OD in PD with involvement of all key stakeholders is needed.
Aims and research questions
The aim of this study was to develop a core outcome set for dysphagia interventions in Parkinson’s disease (COS-DIP) involving people living with OD in PD, family members and family caregivers, healthcare professionals working with people with OD in PD and researchers working in this field. Specifically, we aimed to agree on what outcomes should be measured and how and when these outcomes should be measured.
The following research questions were addressed: (1) what are the core outcomes of interest to measure in clinical trials in OD interventions in PD for people with OD in PD, family members/caregivers, healthcare professionals and researchers? (2) How are these outcomes defined? (3) How should these outcomes be measured? (4) When should these outcomes be measured?
Scope of the COS
We devised the COS-DIP primarily for use in future clinical trials. The health conditions covered by the COS are all types and severities of OD and the population all individuals with idiopathic PD regardless of disease severity and duration. The COS focuses on interventions that directly improve swallowing and/or reduce specific physiological risks associated with OD, such as pneumonia, malnutrition or choking.
Methods
Protocol and registry entry
We developed the study in accordance with the COMET Handbook,20 the Core Outcome Set-STandards for Development (COS-STAD) recommendations23 and the guideline on how to select OMIs for outcomes included in a COS by the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) and COMET initiative.24 We registered the study with the COMET database in September 2021, revised it in March 2024 and published the study protocol.25 The Core Outcome Set-STAndards for Reporting26 and the Accurate Consensus Reporting Document27 guidelines were used in this manuscript to report the study.
Participants
Key stakeholder groups included in this study were people living with OD in PD, family members/caregivers with experience of providing care for a family member and/or living with a family member with OD in PD, healthcare professionals with experience of delivering OD interventions for people with PD and researchers with experience of undertaking research on OD interventions in PD. Participants needed to be proficient in English and ≥18 years old. We applied a maximum variation sample through purposive and snowball sampling through relevant organisations, societies, support groups, personal contacts and social media posts. Authors of published OD in PD trials were contacted directly. Consensus meeting participants were people who completed all three rounds of the online Delphi (eDelphi) survey and agreed to take part in such a meeting at the end of Round 3 of the eDelphi survey.
Development of long list of outcomes
The development of the COS-DIP involved several stages as depicted in figure 1.

Overview of stages involved in developing the core outcome set for dysphagia interventions in Parkinson’s disease. COS-DIP, core outcome set for dysphagia interventions in Parkinson’s disease; OD, oropharyngeal dysphagia; OMI, outcome measurement instrument; PD, Parkinson’s disease.
In the preparatory stage, we generated a long list of outcomes for use in the eDelphi survey through two scoping reviews.15 28 We identified 26 OD-related intervention outcomes currently measured in OD studies with control groups in PD15 and three additional OD-related intervention outcomes in OD studies without control groups in PD.28 Based on discussion within the study steering committee (SSC), we added ten further OD-related intervention outcomes.
To identify outcomes that are important to people with OD in PD, family members/caregivers and dysphagia clinicians, we conducted online surveys and subsequent focus groups. Based on the results of these studies, we added six additional outcomes.29 30 The final long list comprised 45 intervention outcomes related to OD in PD (online supplemental material 1).
Supplemental material
Stage 1: outcome prioritisation process
We conducted a three-round eDelphi survey to identify the core outcomes. The long list of outcomes was translated into lay terms with guidance from a lay person living with PD. All outcomes and lay terms were uploaded to the DelphiManager platform (www.comet-initiative.org/delphimanager). Round 1 was piloted by two SLTs and two lay persons. Based on the received feedback, we amended the wording of the instructions to increase comprehensibility. To mitigate potential attrition bias, we sent regular personalised reminder emails about survey completion and current response rates to participants who had not yet completed the current eDelphi round.
Outcome scoring
We asked participants to rate the importance of each outcome on a nine-point Likert scale as recommended by the Grading of Recommendations Assessment, Development and Evaluation Working Group.31 As preset by DelphiManager, scores of one to three indicate ‘not important’, four to six ‘important but not critical’ and seven to nine ‘critically important’. A score of 10 was ‘unable to rate’, and a text field was provided for additional comments. At the end of Round 1, we asked participants to list any missing but important outcomes. Outcomes suggested by at least two participants were added as new outcomes to Round 2.
In Rounds 2 and 3, we asked participants to re-rate the importance of the outcomes based on the feedback provided. This included the participant’s own rating from the previous round and the percentage of each stakeholder group’s rating for each outcome from the previous round. Participants were anonymous to each other. Only participants who rated all outcomes in one round were invited to take part in the following round.
Consensus definition
Consensus in after Rounds 1 and 2 was defined as ≥70% of all participants scoring seven to nine. After Round 3, consensus was set at ≥60% of all participants scoring seven to nine. All outcomes that did not reach the consensus in criterion were dropped. Outcomes that reached the consensus in criterion formed the list of outcomes for the following round or after Round 3 for the consensus meetings.
Stage 2: agreement on COS-DIP
We conducted two online consensus meetings using the videoconferencing platform Zoom (www.zoom.com) to find consensus on the core outcomes, suggested definitions, OMIs and time points of measurement. Suggested definitions of outcomes were based on previously published definitions, and suggested OMIs were based on validated OMIs for OD in PD, either commonly used in research studies in OD in PD15 or in clinical practice by dysphagia clinicians29 as recommended by Prinsen et al.24 Time points of measurement were suggested based on commonly used time points in research studies15 as well as through the discussion within the SSC. We asked participants whether they agreed (yes/no/unsure) with the final core outcomes, suggested definitions, OMIs and time points of measurement by voting anonymously using Zoom’s polling function. Consensus was defined as ≥70% of participants voting ‘yes’.
By conducting two different consensus meetings, voting on agreement could vary between meetings. To confirm participants’ perspectives, we conducted an anonymous follow-up survey on Qualtrics (www.qualtrics.com), and all previous consensus meeting participants were invited by email to complete the survey. Participants were asked whether they agreed (yes/no/unsure) with the final COS-DIP (online supplemental material 2). We applied the same consensus definition of ≥70% of participants voting ‘yes’.
Supplemental material
Ethics and consent
We obtained ethical approval from the university’s Research Ethics Committee, School of Linguistic, Speech and Communication Sciences, Trinity College Dublin in May 2023 (HT27). Participation in eDelphi was taken as consent. Written and verbal consent was obtained from all participants prior to consensus meetings.
Data analysis
Data on participant demographics and ratings of each outcome in each eDelphi round were analysed descriptively in R (The R Foundation for Statistical Computing, version 4.3.0). We included only data from participants who rated all outcomes in one round. Participants who rated all outcomes identically to each other in one round were excluded. A rating of ‘10’ (unable to rate) was excluded from data analysis for individual outcomes. Feedback on results from previous eDelphi rounds was calculated and displayed in the following round automatically by DelphiManager. Data of the consensus meetings were analysed descriptively in Excel (Version 16.87).
Patient and public involvement
The project was overseen by a SSC that included three SLTs, a neurologist, a COS expert and an individual living with PD. The individual with PD was involved in all stages of the research process: the design and review of the eDelphi surveys, the consensus meetings, recruitment of participants and dissemination of results, thereby enhancing the accessibility, understandability and validity of this study.20
Results
Protocol deviations
Deviations made from the study protocol and the corresponding reasons for these changes are available in online supplemental material 3.
Supplemental material
Participants
133 participants registered via DelphiManager, 114 completed Round 1, 104 completed Round 2 and 90 completed Round 3. This represents a response rate of 91% between Rounds 1 and 2 and 87% between Rounds 2 and 3. Numbers and percentages of participants in each stakeholder group who dropped out are depicted in online supplemental material 4. One participant was excluded due to rating all outcomes in all rounds with a score of nine. 90 participants were from 21 countries and represented all three stakeholder groups. Participants’ demographics for each eDelphi round are displayed in table 1.
Supplemental material
Characteristics of participants in each eDelphi round
Of the 90 participants who completed Round 3, 50 agreed to participate in a consensus meeting. Of these, 35 attended one of the two subsequent consensus meetings (table 2).
Demographics of participants in each consensus meeting
We invited all 35 consensus meeting participants to participate in the anonymous follow-up survey. Of these, 26 participants completed the survey. Sociodemographic data from survey participants was not collected to keep the burden on respondents as low as possible.
Stage 1: outcome prioritisation process
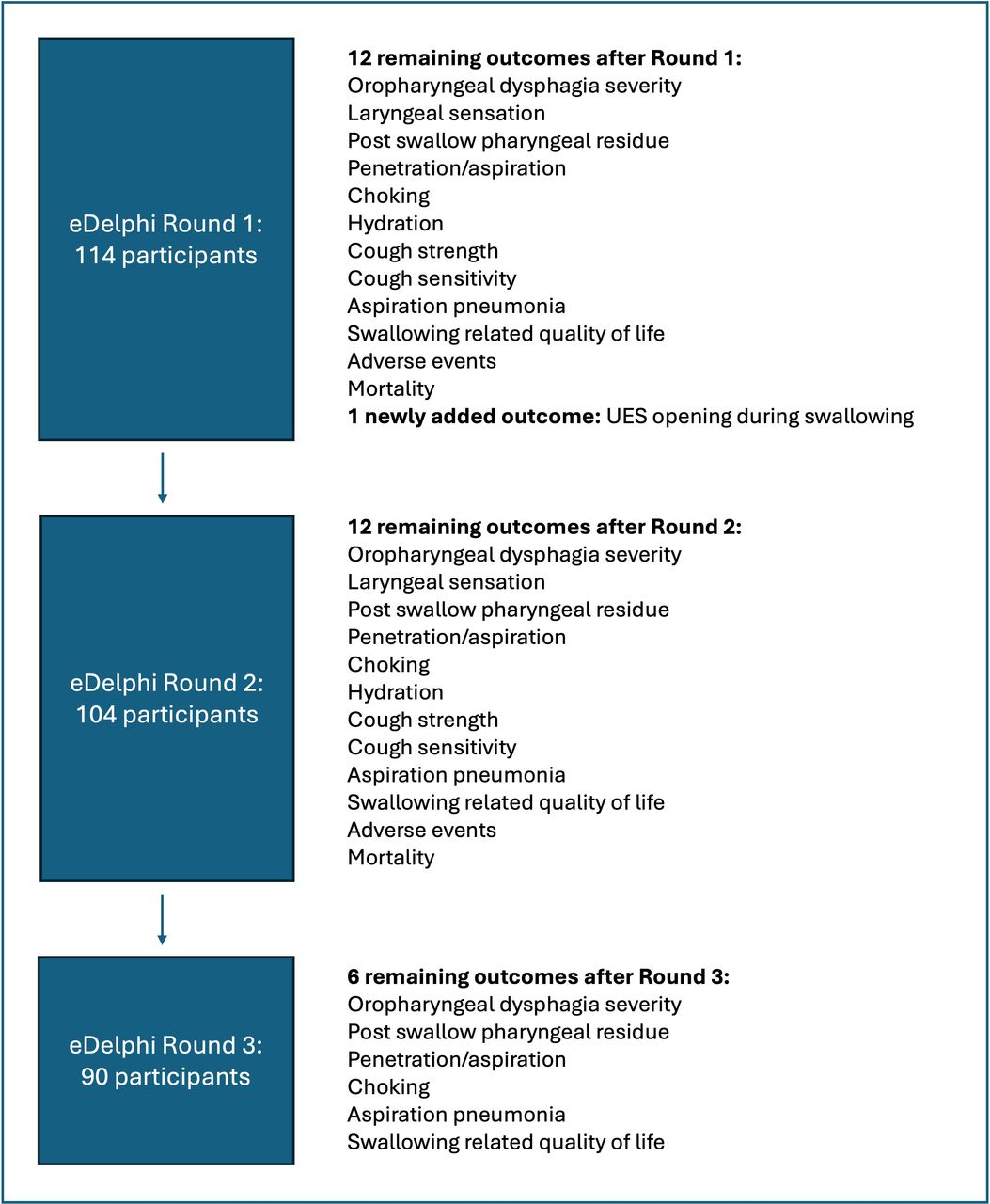
Overall, participants indicated that they were ‘unable to rate’ (score of 10) 4.6% of outcomes in Round 1, 2.4% in Round 2 and 1.6% in Round 3. Most participants did not provide a reason for choosing this score. Due to the exclusion of these ratings, the overall number of participants’ ratings differs between outcomes. Online supplemental material 5 depicts the number of participants using a rating of 10 for each of the three rounds. In addition, we found that people with OD in PD and family members/caregivers requested more support via email to log in to DelphiManager and access the eDelphi rounds than healthcare professionals/researchers. Figure 2 outlines the prioritisation process through the three round eDelphi surveys with the numbers of participants per round and the retained outcomes per round.
Supplemental material

{kind=link}
{kind=link}
Outcome prioritisation process through three-round eDelphi survey. eDelphi, online Delphi; UES, upper oesophageal sphincter.
Round 1 was open from 10 January to 3 February 2024, and 45 outcomes were included. Of these, 33 did not reach consensus and were dropped after this round. No outcome was rated ‘critically important’ (scores 7–9) by ≥70% of participants in each stakeholder group individually. The outcome ‘laryngeal sensation’ was rated ‘critically important’ only by ≥70% of people with PD (n=16, 76%). The outcomes rated most frequently ‘critically important’ by family members/caregivers were ‘choking’ (n=8, 89%) and ‘penetration/aspiration’ (n=7, 88%). The outcomes rated most frequently ‘critically important’ by healthcare professionals/researchers were ‘penetration/aspiration’ (n=78, 99%), ‘aspiration pneumonia’ (n=72, 92%) and ‘OD severity’ (n=72, 91%).
In total, participants provided 49 suggestions for additional outcomes in Round 1. Only ‘upper oesophageal sphincter (UES) opening during swallowing' met the criterion for inclusion in the next round and was therefore added as an outcome to the remaining 12 outcomes from Round 1, resulting in 13 outcomes for Round 2.
Round 2 was open from 14 February to 12 March 2024. The newly added outcome ‘UES opening during swallowing’ did not reach consensus and was dropped. All other outcomes were retained for Round 3. The outcomes ‘penetration/aspiration’ and ‘choking’ were rated as ‘critically important’ by ≥70% of participants in each stakeholder group individually. To 70% (n=14) of people with PD, the outcome ‘mortality’ was also ‘critically important’. ‘OD severity’ (n=7, 88%) and ‘laryngeal sensation’ (n=5, 71%) were ‘critically important’ to ≥70% of family members/caregivers. To healthcare professionals/researchers, all outcomes except for ‘UES opening during swallowing’ were ‘critically important’ to ≥70%. Particularly ‘penetration/aspiration’ (n=73, 99%), ‘aspiration pneumonia’ (n=70, 96%) and ‘OD severity’ (n=70, 95%) were rated most frequently as ‘critically important’ by this stakeholder group.
Round 3 was open from 27 March to 19 April 2024. Of the 12 outcomes in Round 3, six outcomes were dropped due to not reaching consensus. The six remaining outcomes were ‘penetration/aspiration’ (n=75, 83%), ‘aspiration pneumonia’ (n=65, 73%), ‘choking’ (n=60, 67%), ‘OD severity’ (n=57, 65%), ‘swallowing related quality of life’ (n=56, 62%) and ‘post swallow pharyngeal residue’ (n=54, 61%).
The outcomes ‘penetration/aspiration’ and ‘choking’ were rated as ‘critically important’ by ≥60% of participants in all three stakeholder groups. No other outcome was rated as ‘critically important’ by ≥60% of family members/caregivers, whereas the outcome ‘mortality’ was ‘critically important’ to ≥60% of people with PD (n=11, 65%). All six remaining outcomes were ‘critically important’ to ≥60% of healthcare professionals/researchers. Online supplemental material 6 provides all absolute numbers and percentages of 7–9 ratings for all three stakeholder groups individually and together. Online supplemental material 7 comprises all outcomes and definitions that were uploaded to each round to DelphiManager.
Supplemental material
Supplemental material
Stage 2: agreement on COS-DIP
We conducted two online consensus meetings in May 2024. All six core outcomes were agreed on by 82% of consensus meeting participants. Of the remaining participants, 9% voted ‘no’ or ‘unsure’, respectively. Definitions and OMIs were discussed within the consensus meetings and agreed on by participants. An overview of the definitions and OMIs presented for discussion by the SSC and the suggested changes made by consensus meeting participants is provided in online supplemental material 8.
Supplemental material
Time points for measurement suggested by the SSC in the consensus meetings were as a minimum immediately before the start of the intervention, immediately after and 3 months after completion of intervention. Additionally, measurements 1 month before and 6 and 12 months after completion of the intervention were recommended. In the first consensus meeting, 83% (n=15) of the participants agreed on these time points of measurement. In the second consensus meeting, it was suggested to only have a pre- and post-assessment as a minimum and change the term ‘recommended’ to ‘advisable’. This was agreed on by 69% (n=9) participants in this meeting. After discussion within the SSC, we amended the wording as suggested in the second meeting. However, as the absolute number of participants in the first meeting was higher than in the second meeting, no changes for the time points of measurement were made.
For the follow-up survey, we incorporated the suggested changes by consensus meeting participants into the definition of choking and OMIs for ‘penetration/aspiration’, ‘OD severity’ and ‘post swallow pharyngeal residue’. Agreement on six core outcomes, definitions, OMIs and time points of measurement was achieved. Table 3 depicts the agreed core outcomes, definitions and OMIs.
Core outcomes with definitions and measurement(s) agreed on by consensus meeting and follow-up survey participants
The agreed minimum time points of measurement are before the start and at the end of intervention and 3 months post-completion of intervention. The agreed advisable, additional time points of measurement are 1 month before the start and 6 and 12 months post-completion of intervention.
Discussion
This study developed the first COS for OD interventions in people with PD. Consensus was reached on six core outcomes. Definitions, OMIs and time points of measurement were established and agreed for all six core outcomes.
Core outcomes
The six core outcomes agreed in this study were largely consistent with previous research. ‘Penetration/aspiration’, ‘OD severity’, ‘swallowing related quality of life’ and ‘post swallow pharyngeal residue’ are outcomes previously considered important by all key stakeholder groups based on surveys29 30 and are frequently measured by researchers in OD in PD studies.15 ‘Penetration/aspiration’ is the outcome that is clearly considered the most important outcome in OD intervention studies in PD by all three stakeholder groups and shows the largest agreement.
OMIs
There is a huge variety of OMIs to measure OD-related outcomes. However, some are not validated for PD specifically or are overly long and not user friendly (eg, SWAL-QOL32). Further, there is a lack of agreement on diagnostic criteria for pneumonia.33 34 The suggested measurement for pneumonia was agreed on by consensus meeting participants in both COS studies on intensive care35 and this one for OD in PD, as well as criteria suggested by Robbins et al.36
In published research studies in OD in PD, ‘penetration/aspiration’ and ‘swallowing related quality of life’ were the outcomes measured most consistently using the Penetration-Aspiration Scale37 and SWAL-QOL,32 respectively. In contrast, ‘OD severity’ is being measured differently,15 which needs to be addressed in future research. Scales used with instrumental assessment, such as VASES38 and DIGEST-FEES,39 have only been developed or validated for PD after completion of the scoping review15 and are therefore not yet used in the included OD intervention studies in PD. However, due to their established validity and comprehensive outcome assessment, we believe that they are likely to be useful OMIs in future clinical trials. The measurement of ‘choking’ poses a challenge as no validated OMI exists so far. It is, therefore, essential to develop a valid and reliable OMI for choking.
Time points of measurement
In a neurodegenerative condition like PD, long-term follow-up assessments are critical. The longest follow-up assessment in studies included in the scoping review was 6 months after completion of the intervention.15 Considering the core outcome ‘aspiration pneumonia’ and its delayed potential development of post-aspiration events, longer-term follow-ups, as advised in the COS-DIP, are needed. The explicit specification of time points of measurement in this COS provides crucial guidance for future trials, further enhancing the comparability of results across studies and enabling more meaningful meta-analyses.
Challenges in COS research
It is important that a COS is widely adopted; otherwise, it will add to research waste rather than facilitate its reduction.18 In a systematic review on the uptake of the COS for PD by de Roos et al21 in RCTs, the problems of multiple outcomes not being measured and a high variety of OMIs used were identified.40 This is in line with other studies that have identified barriers to the uptake of COS, such as a lack of awareness and knowledge of COS and how to find and measure the core outcomes.41–43 Ongoing dissemination of the COS-DIP to raise awareness among clinical trialists, funders and people with the health condition is key to its adoption and integration into clinical trials. Additionally, the COS-DIP should be seen as a living document that needs to be revised and updated once new information (eg, experience with using the COS in research or new, validated OMIs) emerges.
Strengths and limitations
A strength of this study is the novel approach to developing the long list of outcomes by conducting online surveys with people with OD in PD, family members/caregivers and dysphagia clinicians. This ensured that all perspectives were included in the development of the long list of outcomes prior to the eDelphi survey. An additional strength is the inclusion of key stakeholders from previously underserved groups, with a large geographical coverage, representing a wide range of different perspectives, making it more relevant to all stakeholder groups. This is despite the study being in English and online only. Furthermore, this COS achieved consensus on the OMIs and time points of measurement for the core outcomes. While many COS studies focus primarily on what to measure, this COS also addresses how and when to measure outcomes, providing comprehensive guidance for future clinical trials in this field.
One limitation of this study was the relatively small number of people with OD in PD and family members/caregivers compared with healthcare professionals/researchers. Due to the small sample size, the ratings per eDelphi round need to be interpreted with caution. One potential reason for this smaller sample size is both the online format as well as the use of the DelphiManager platform that might have posed challenges to these two groups. This became evident in the increased number of email requests for assistance from the research team. For future COS studies planning on using DelphiManager, it would be advisable to have the option of bigger font for people with visual impairment, to have adapted website formats to different devices (computer, tablet and smartphone) and to improve the log-in process to the website. This would reduce the burden of participants and potentially increase participation and retention rates.
Despite these challenges, proportionately more people with the health condition and family members/caregivers were included in this study compared with other COS studies in dysphagia. In the COS for patient-reported dysphagia in head and neck cancer clinical trials, nine of the 45 participants were people with the health condition and family members.44 The COS for dysphagia intervention outcomes in intensive care included a total of 160 participants, with 18 people with the health condition and no family members/caregivers.35
Participant attrition between Delphi rounds is a common challenge that requires careful consideration.20 Although we achieved response rates of 91% and 87% between Rounds 1 and 2, respectively, those who did not complete all rounds or submitted incomplete responses may have held different views. This potential selection bias could influence the final consensus if participants with certain perspectives were more likely to drop out. However, our analysis showed there was no particular stakeholder group that had a significantly higher attrition rate between the two rounds than any other stakeholder group. Additionally, the strong consensus achieved in the final COS-DIP suggests that any impact of participant attrition was likely minimal.
Conclusions
This COS for OD interventions in PD was developed by key stakeholder groups, including people living with the health condition, and consists of six core outcomes. These comprise ‘penetration/aspiration’, ‘aspiration pneumonia’, ‘choking’, ‘OD severity’, ‘swallowing related quality of life’ and ‘post swallow pharyngeal residue’. To ascertain that outcomes remain relevant and important to all key stakeholders, the COS-DIP should be regularly reviewed as a means of validation. Additionally, it is important to assess if and how the COS-DIP is measured and reported in future OD intervention studies in PD. Future research should focus on (1) evaluating the uptake of the COS-DIP in clinical trials, (2) assessing whether its use improves the quality and comparability of systematic reviews and meta-analyses in this field and (3) investigating potential barriers to its implementation in different research settings. Ultimately, this COS contributes to improving the evidence base for OD interventions in PD, which may result in a clearer direction on what intervention works best for OD in PD.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this published article and its supplementary material.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. We obtained ethical approval from the university’s Research Ethics Committee, School of Linguistic, Speech and Communication Sciences, Trinity College Dublin in May 2023 [HT27]. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to acknowledge the support of all organisations, societies and clinicians who helped in recruiting participants. We would like to thank all participants for taking part in the Delphi survey and consensus meetings. Permission was granted to acknowledge the following Delphi survey participants by name: Adriaan Esterhuizen, Dina Roos, Johanna Weitzel, Lawrence Graham Cross, Bente van der Sluis, Dharshini, Anna Tucker, Adele Kay, Caoimhe Hunter McGowan, Catriona Steele, Angi Pendreich, Almut Niessen, Bernadette Carroll, Andrea Hofmayer, Grazia Leanza, Kerstin Erfmann, Liam Lynch, Gillian Palmer, James Curtis, Numan Demir, Lynette Bryan, Pooja Gandhi, Denise Pighetti, Susanne Javorszky, Irene Battel, Rob Smith, Bendix Labeit, Karen Baldwin, Julie Regan, Nicole Herndon, Anne Rittié Burkhard, Christine Wallace, Emma Wallace, Bill Merrill, Lucilla, Michel van Hooren, Corinne Jones, Sonja Suntrup-Krüger, Ivy Cheng, Rebecca Oldenburg, Cornelius Werner, Andrew Shedden, Alison Coats, Katharina Winiker, Josh Fijten, Pat Martin, Anna Gillman, Helen Brake, Terence Broomfield, Edward Carter, Patricia, Sabrina Hetterich, Jill Gaylor, Ayodele Sasegbon, Joanne Keenan, Daniela Filipa Brás Ferreira, Maria Valeria Levi Della Vida, Olwen O'Meara, Eoin Lynch, William Hughes, Björn Degen, Pere Clavé, Stefanie Duchac, Orla Maher, Arianna Caselli, Katrin Eibl, Julia Glinzer and Sarah Perry.
References
Footnotes
Deceased MW since deceased.
Contributors JH designed, conducted and analysed the Delphi survey and consensus meetings and drafted the manuscript. GB and TW are part of the study steering committee and advised the design and conduct of the Delphi survey and consensus meetings. PC is part of the study steering committee and is the secondary supervisor of this research project. MW conceptualised the study, co-conducted the consensus meetings and was the primary supervisor of this research project. MW is responsible for the overall content as guarantor. All authors critically appraised and edited the manuscript. All authors read and approved the final manuscript.
Funding JH is funded through a Provost’s PhD Award from Trinity College Dublin, Ireland. The costs for using the DelphiManager platform were funded by a TRiSS postgraduate research fellowship by Trinity College Dublin, Ireland.
Disclaimer The funding bodies do not have any role in this study.
Competing interests TW has received honoraria from BIAL, Abbvie, Desitin, Zambon, Pfizer, Britannia, Esteve and Licher; consultancies from Desitin, BIAL, Stadapharm and Phagenesis; and funding from Abbvie and EVER Pharma.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.